
It consists of two separate articulations:
Note: The proximal radioulnar joint is found within same joint capsule of the elbow, but most resources consider it as a separate articulation.
Like all synovial joints, the elbow joint has a capsule enclosing the joint. This in itself is strong and fibrous, strengthening the joint. The joint capsule is thickened medially and laterally to form collateral ligaments, which stabilise the flexing and extending motion of the arm.
A bursa is a membranous sac filled with synovial fluid. It acts as a cushion to reduce friction between the moving parts of a joint, limiting degenerative damage. There are many bursae in the elbow, but only a few have clinical importance:
The joint capsule of the elbow is strengthened by ligaments medially and laterally.
The radial collateral ligament is found on the lateral side of the joint, extending from the lateral epicondyle, and blending with the annular ligament of the radius (a ligament from the proximal radioulnar joint).
The ulnar collateral ligament originates from the medial epicondyle, and attaches to the coronoid process and olecranon of the ulna.
The arterial supply to the elbow joint is from the cubital anastomosis, which includes recurrent and collateral branches from the brachial and deep brachial arteries.
Its nerve supply is provided by the median, musculocutaneous and radial nerves anteriorly, and the ulnar nerve posteriorly.
The orientation of the bones forming the elbow joint produces a hinge type synovial joint, which allows for extension and flexion of the forearm:
Note – pronation and supination do not occur at the elbow – they are produced at the nearby radioulnar joints.
Subcutaneous bursitis: Repeated friction and pressure on the bursa can cause it to become inflamed. Because this bursa lies relatively superficially, it can also become infected (e.g cut from a fall on the elbow)
Subtendinous bursitis: This is caused by repeated flexion and extension of the forearm, commonly seen in assembly line workers. Usually flexion is more painful as more pressure is put on the bursa.
An elbow dislocation usually occurs when a young child falls on a hand with the elbow flexed. The distal end of the humerus is driven through the weakest part of the joint capsule, which is the anterior side. The ulnar collateral ligament is usually torn and there can also be ulnar nerve involvement
Most elbow dislocations are posterior, and it is important to note that elbow dislocations are named by the position of the ulna and radius, not the humerus.
Most of the flexor and extensor muscles in the forearm have a common tendinous origin. The flexor muscles originate from the medial epicondyle, and the extensor muscles from the lateral. Sportspersons can develop an overuse strain of the common tendon – which results in pain and inflammation around the area of the affected epicondyle.
Typically, tennis players experience pain in the lateral epicondyle from the common extensor origin. Golfers experience pain in the medial epicondyle from the common flexor origin. This is easily remembered as golfers aim for the ‘middle’ of the fairway, while tennis players aim for the ‘lateral’ line of the court!
A supracondylar fracture usually occurs due to a fall onto on outstretched, extended hand in a child (95%) but more rarely can occur by a direct impact onto a flexed elbow. It is typically a transverse fracture, spanning between the two epicondyles in the relatively weak epicondylar region formed by the olecranon fossa and coronoid fossa which lie opposite each other in the distal humerus.
Direct damage, or swelling can cause the interference to the blood supply of the forearm via the brachial artery. The resulting ischaemia can cause Volkmann’s ischaemic contracture – uncontrolled flexion of the hand, as flexors muscles become fibrotic and short. There also can be damage to the medial, ulnar or radial nerves. As a result, the neurovascular examination and documentation of all patients presenting with these injuries is vital. Sometimes, the blood supply can be interrupted acutely leading to a ‘pale, pulseless’ limb often in a child, usually requiring emergency surgery.

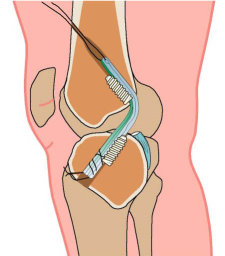
Elbow arthroscopy is keyhole surgery of the elbow. It can be used to treat a number of conditions inside the joint. It can be used in conjunction with physiotherapy to improve the range of movement of a stiff joint.
Rest is the treatment of choice when the pain first appears. If the pain is severe, short term immobilisation of the arm in a splint may be helpful in some patients. This rest aims to allow the tiny tears in the tendon attachment to heal.
‘Golfers elbow’ is a condition where the inner part of the elbow becomes sore and tender. Although commonly associated with golf the condition can affect almost anybody. The condition is also known as medial epicondylitis, although histologic studies have shown no evidence of an inflammatory process.
‘Tennis elbow’ is a condition where the outer part of the elbow becomes sore and tender. Although commonly associated with tennis and other racquet sports the condition can affect almost anybody. The condition is also known as lateral epicondylitis, although histologic studies have shown

5000

1000
10000

750

